It may be possible to remove your bile duct cancer with surgery if it is found at an early stage. That means it is completely contained within the bile ducts, or has grown just outside them. Your doctor may describe your cancer as ‘resectable’. Completely removing the cancer with surgery may cure it.
Surgery to completely remove the cancer isn’t possible (it is ‘unresectable’) if your tests show that it’s spread to nearby body tissues or other body organs. Unfortunately, only about 2 out of every 10 bile duct cancers (20%) are resectable.
Whether you can have surgery also depends on:
- the results of all your tests
- how fit you are
- whether you have any other medical conditions that could cause problems with your recovery
Removing bile duct cancer is highly skilled surgery. So you’ll need to be referred to a surgeon who specialises in carrying out this type of operation. It’s also a major operation, which is why your health team will need to take your general health into account.
Your surgeon will aim to remove the cancer with a border of healthy tissue around it, so there are no cancer cells left behind. Doctors call this a ‘clear margin’.
The type of operation
The exact operation you have will depend on :
- exactly where the cancer is in the bile ducts
- the size of the cancer
- whether it has broken through the wall of the bile duct
Intrahepatic bile duct cancer – removing part of your liver
If you have intrahepatic bile duct cancer, the affected bile ducts are all inside the liver. To remove the cancer, your surgeon will have to take out the section of your liver than contains them. This is called a liver resection.
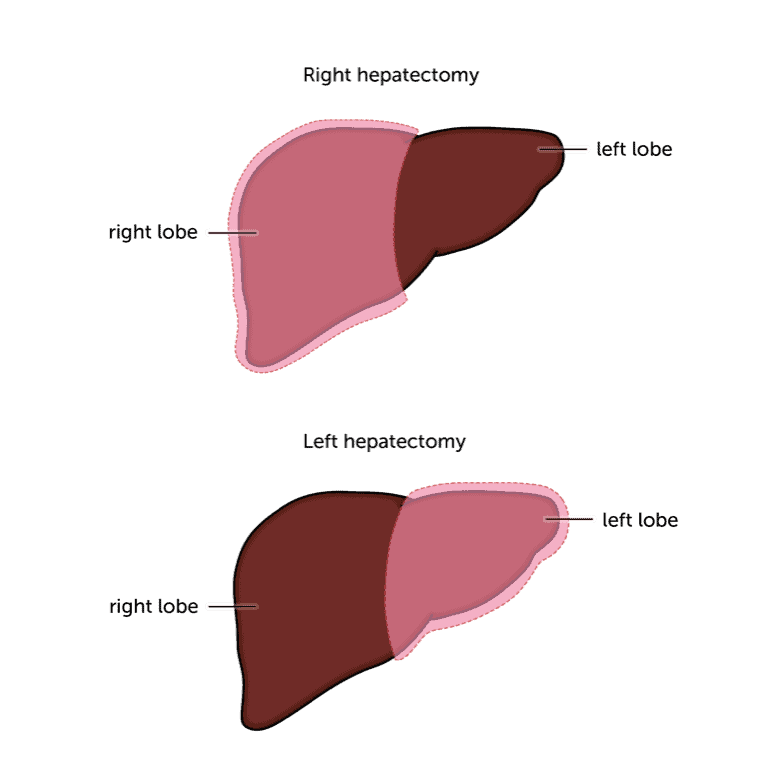
The liver is made up of two lobes – right and left. Sometimes, it may be necessary to remove a complete lobe. This is called a lobectomy.
The liver is unique in the body, in that it can grow back. So having part of it removed isn’t a problem as long as your liver is reasonably healthy. If you have another liver condition, such as cirrhosis, your doctor will check how well your liver is working before deciding whether you can have the surgery.
There is more detail about having a liver resection and other types of surgery in our liver cancer surgery section.
Extrahepatic bile duct cancer
If you have extrahepatic bile duct cancer – either perihilar or distal – you are likely to need a bigger operation. Exactly what your surgeon needs to remove depends on where the cancer is growing. A few people with very early bile duct cancer may be able to have just the bile ducts removed, but it isn’t common.
Having just the bile ducts removed
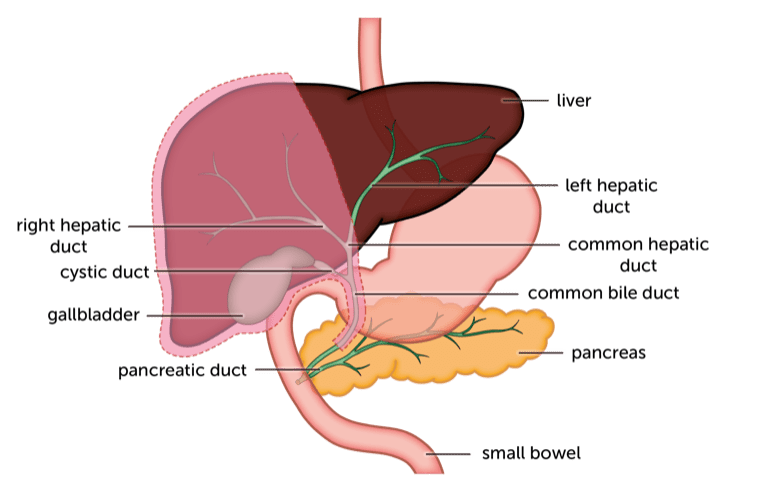
In a very small number of patients, the cancer is found early enough for the surgeon to be able to remove just the external bile ducts and nearby lymph nodes. The surgeon will join the gallbladder to the small bowel so bile can still flow.
Peri-hilar cancer
The external bile ducts are very close to a number of other body organs, including the pancreas, small bowel and stomach. To lower the risk of the cancer coming back, your surgeon will remove parts of these organs that are nearest to the cancer.
As with a very early bile duct cancer, your surgeon will need to remove the bile ducts outside the liver and all the lymph nodes nearby. You will also have your gallbladder and part of your liver removed.
Distal cancer
If you have distal bile duct cancer, you may need to have part of your pancreas and the first part of your small bowel (the duodenum) removed as well as the bile ducts and nearby lymph nodes. The surgeon will join your liver, stomach and remaining pancreas to the second part of your small bowel (the jejunum).
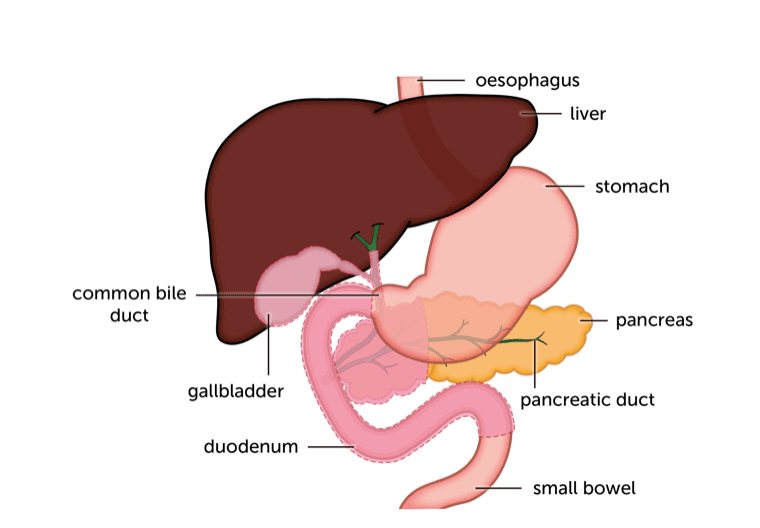
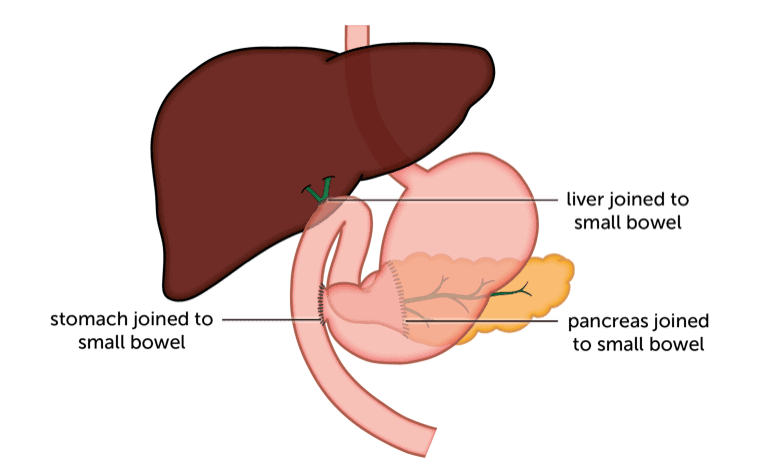
This operation is called a pancreatoduodenectomy (say: pank-ree-at-oh dew-oh-den-ek-tom-ee). You may also hear it called a ‘Whipple procedure’, which is just an old name for the same thing.
There is more information about having a pancreatoduodenectomy and other types of surgery in our liver cancer surgery
section.
Treatment after surgery
After your operation, your doctor may suggest a course of chemotherapy. This helps to lower the risk of the cancer coming back. Doctors call this adjuvant treatment (say: ad-joo-vent).
You are most likely to have tablets of a chemotherapy drug called capecitabine (say: cap-site-a-been). You take these daily for 2 weeks and then have a week off. This 3-week period is called a cycle of treatment. You usually have treatment for 6 months (around 8 cycles) after your surgery.
Like all chemotherapy drugs, capecitabine does have some side effects. In a clinical trial researching the use of capecitabine after bile duct cancer surgery, the commonest side effects were:
- hand and foot syndrome in 20 out of 100 people (20%)
- diarrhoea in 8 out of 100 people (8%)
- fatigue in 8 out of 100 people (8%)
Hand and foot syndrome is also called palmar-plantar erythema (say: eh-rith-eh-ma). Erythema just means redness. It causes sore, red and peeling skin on the palms of the hands and soles of the feet. You may also have numbness and tingling.
Side effects usually get better a couple of weeks after your course of treatment ends.
There is more about chemotherapy in our main liver cancer treatment section.
Liver transplant
A UK liver transplant unit is being set up for patients with bile duct cancer and underlying chronic liver disease. Only patients with early disease, small tumours, with no sign of spread outside the liver can have this type of treatment. If your specialist thinks it’s suitable for you, they can refer you to a transplant centre for assessment.
You can read detailed information about liver transplants on the main British Liver Trust website.
Content last reviewed: October 2022
Next review date: October 2025