Early stage HCC means your Barcelona stage is either 0 or A. You may have between 1 and 3 small tumours in your liver and you are otherwise well.
Your specialist may suggest treatment with:
- surgery to remove a single liver tumour (resection)
- a liver transplant
- thermal ablation to destroy a tumour with heat – using either radio waves (RFA) or microwaves
- Embolization or TACE – blocking the tumour’s blood supply (embolization) which may be combined with chemotherapy (TACE)
- Embolization with radiation (SIRT or TARE)
- External stereotactic radiotherapy (SABR)
Surgery to remove a liver tumour
For a single liver tumour, this is the treatment you’re most likely to have. Your doctor may call it a liver resection. They will remove the part of the liver containing the cancer. The aim of the treatment is to cure your liver cancer.
Whether you can have a liver resection depends on:
- the size of the tumour
- where it is and whether it has grown into blood vessels
- how well your liver is working
The liver is made up of two lobes – right and left. Sometimes, it may be necessary to remove a complete lobe. This is called a lobectomy.
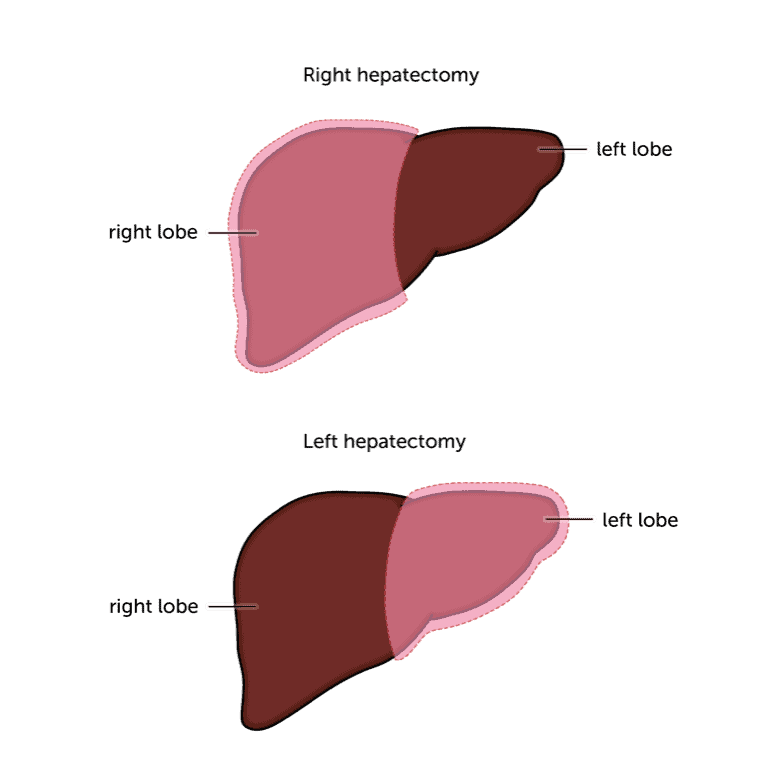
Because the surgeon will be removing part of your liver, they need to make sure that the remaining liver is working well enough. The liver is unique in being able to grow back after part of it has been removed. So having part of it removed isn’t a problem as long as your liver is reasonably healthy. But if you have other liver disease, apart from the cancer, you may be too unwell afterwards to make a good recovery. So this type of surgery won’t be possible.
Unfortunately, fewer than 1 in 3 people (around 30%) will be able to have this type of treatment because they have other liver disease or their HCC had grown too far before it was found.
If you have fibrolamellar HCC you are more likely to be able to have surgery. This type of HCC often affects people who don’t have any other type of liver disease. If your remaining liver tissue is healthy, your liver will be able to grow back.
There is more information in our general treatment sections, including information on preparing for surgery and what happens after your operation.
Liver transplant
Your doctor may suggest a liver transplant if other liver disease means your liver wouldn’t work well after you’ve had part of it removed. The aim of the surgery is to try and cure your liver cancer.
Whether you can have a transplant depends on how many tumours there are and how big they are. Generally, you can have a transplant if you have a single tumour less than 5cm across, or up to 5 tumours less than 3cm across. The cancer can’t have grown into blood vessels or spread outside the liver.
To qualify for a transplant, you also need to meet the UK Transplant Criteria. There should be no other suitable treatment (those described on this page) that could cure your cancer. If you’ve ever had a problem with heavy drinking or intravenous (IV) drug use, you have to sign an agreement that you’ll stop. If this is the case, you’ll have regular alcohol or drug testing while you’re on the transplant list. Everyone will have regular scans to make sure the cancer isn’t growing too much.
Of course you also need a donor, which can take time. You might need to have other treatments to help control the growth of the cancer while you wait.
A transplant is major surgery. Although you can have it if you have liver disease, you need to be generally fit and well enough to recover. Your doctor may refer you to a transplant unit, who will check that you’re fit enough. They will take into account any other illnesses or medical conditions you have.
There is more about liver transplant on the main British Liver Trust website.
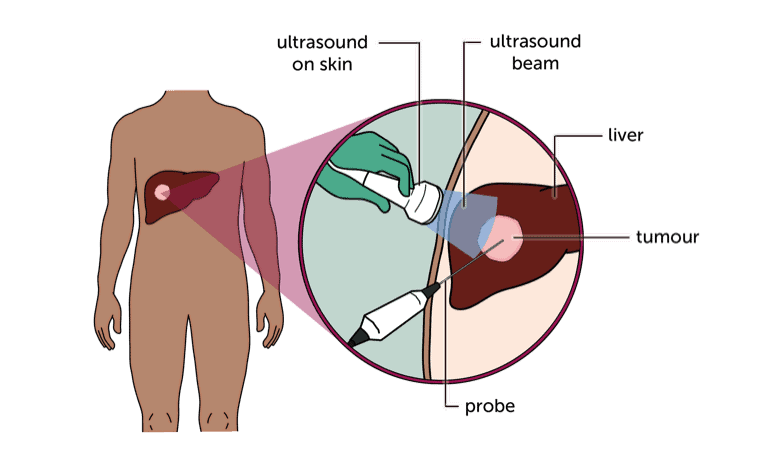
Thermal ablation (RFA or microwave)
Thermal ablation means destroying tumours with heat. Your doctor can do this either with radio waves (radiofrequency ablation or RFA) or microwaves. You have an ultrasound scan during the procedure, which the doctor uses to guide the probe.
Your doctor may suggest this type of treatment if there are reasons why surgery isn’t suitable for you, or if they think it would be a better option in your case.
For early HCC, the aim is to try and cure the cancer. But if you are waiting for a transplant, your doctor may also use it to try and control the cancer until a suitable donor liver becomes available.
Whether you can have ablation to try and cure HCC depends on:
- the size and number of tumours
- where they are
- how well your liver is working
You usually only have RFA for a single tumour, but you can have it for more than one. It works very well for tumours smaller than 3cm and is likely to completely destroy them. If the tumour is very near something that could be damaged by heat (such as a major blood vessel or the gallbladder) your doctor won’t recommend thermal ablation. They may suggest radiotherapy instead.
There is more information about having thermal ablation in the general liver cancer treatment section.
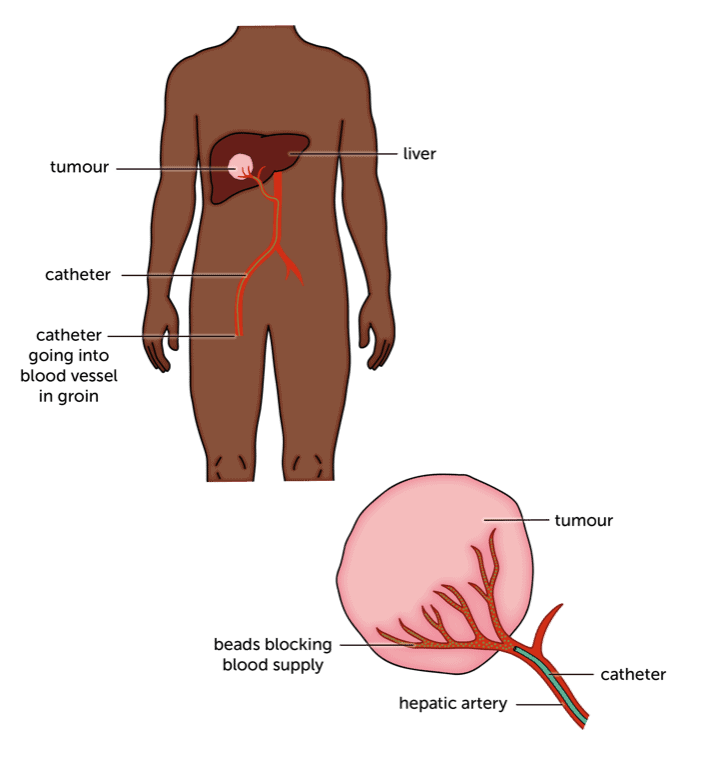
Embolization and TACE
Embolization means blocking the blood supply to the cancer. This starves the cancer cells of food and oxygen, which would normally be carried to them in the blood.
TACE stands for Trans Arterial Chemo Embolisation. It combines chemotherapy with embolization.
Your doctor may suggest this type of treatment if you are waiting for a transplant. The aim is to keep the cancer under control until a suitable liver becomes available.
For embolization, the doctor will inject tiny beads to block the blood vessels that supply the tumour. Starved of food and oxygen, the tumour will then shrink.
For TACE, the doctor injects the chemotherapy directly into the blood supply to the liver. The chemo is mixed with a fatty oil that keeps it in the tumour. Then you have the beads injected to block off the blood supply to the cancer. Sometimes doctors use beads that contain the chemo drug. So it delivers the chemo and blocks the blood supply in one go.
Because the chemo goes straight to the liver, TACE doesn’t have the side effects that you may associate with chemo. But you may have some side effects from the embolization, including a temperature, aches and pains and tiredness.
TACE is usually a single treatment. You’ll have scans afterwards, to check how well it’s worked. You can have TACE several times, over months or years if necessary.
There is more about embolization and TACE in the general liver cancer treatment section.
Embolization with radiation – SIRT or TARE
This is a treatment similar to TACE. It’s a type of internal radiotherapy, combined with blocking the tumour’s blood supply. SIRT and TARE are different names for the same thing. SIRT stands for ‘Selective Internal Radio Therapy’. TARE stands for ‘Trans Arterial Radio Embolization. The aim of the treatment is to try and cure the cancer.
The doctor places tiny radioactive beads into the blood supply around the tumour. The beads work in two ways. They deliver radiation to the tumour, which kills the cancer cells. And the beads block the small blood vessels around the tumour, cutting off its blood supply. This starves it of food and oxygen.
There is more information about how you have SIRT (or TARE) in the section on liver cancer treatment.
External (stereotactic) radiotherapy (SABR)
If you can’t have surgery, your doctor may suggest stereotactic radiotherapy to destroy a liver tumour. This is also called radiosurgery, ‘gamma knife’ or ‘cyberknife’. It’s also sometimes called stereotactic body radiotherapy (SBRT) or stereotactic ablative radiotherapy (SABR). They all mean the same thing.
This is a highly targeted form of radiotherapy where several beams are directed at the cancer from different directions. This allows the doctor to target the treatment really accurately, so they can use higher doses of radiation to destroy a tumour completely.
There is more information about having radiotherapy in our general information on liver cancer treatment.
Content last reviewed: October 2022
Next review date: October 2025